
When machine learning meets lived clinical wisdom, complex dizziness finally gets an 88 percent answer key.
1. Introduction: A Puzzle That Would Not Sit Still
Imagine waking up and the room tilts in slow motion. You grip the bedframe, hoping gravity will pick a direction and stay there. Dizziness and vertigo are deceptively common, yet the underlying causes bounce across more than two dozen vestibular disorders. Seasoned specialists spend years learning to untangle them. General practitioners often feel like they are spinning the stethoscope wheel of fortune.
This uncertainty ripples far beyond the clinic. Misdiagnosis sends patients on expensive diagnostic scavenger hunts. Delayed treatment fuels anxiety. Hospitals burn time on follow-up appointments that might never have been needed.
Enter AI medical diagnosis, a field racing to turn raw patient data into crisp clinical direction. Over the past decade, machine learning in medicine has cracked radiology, dermatology, and even pathology slides. But vestibular disorders remained elusive—too many overlapping symptoms, not enough large datasets, and a persistent fear that algorithms might miss life-altering red flags.
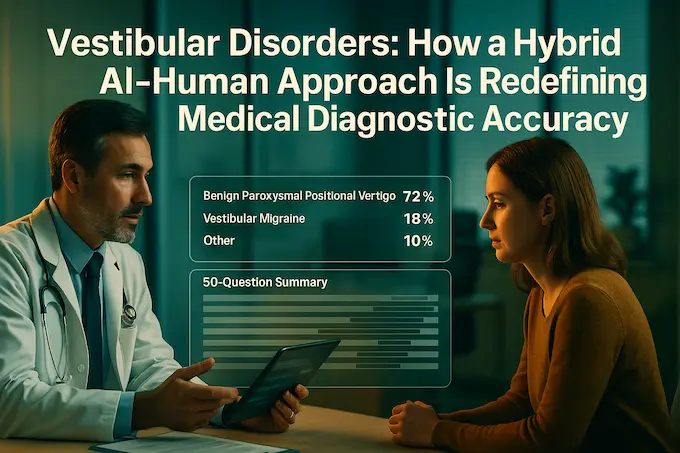
A new study published last week in npj Digital Medicine flips that narrative. A Seoul-based team combined CatBoost gradient boosting with “lived experience coaching,” a fancy phrase for veteran specialists guiding the model like flight instructors. The result: an AI medical diagnosis system that scores 88.4 percent overall accuracy while maintaining surgical specificity on the scariest conditions. In other words, it catches the common culprits and flags the dangerous outliers without triggering a cascade of unnecessary tests.
The project is more than another accuracy benchmark. It maps a practical blueprint for AI in healthcare that honors human judgment instead of elbowing it aside. Think of it as Sully Sullenberger letting the Airbus autopilot handle cruise altitude while he keeps a hand on the yoke for takeoff and landing.
Table of Contents
2. Why Vestibular Disorders Break Traditional Checklists
Vestibular disorders love to masquerade as each other, a diagnostic costume party inside the inner ear. Doctors must juggle the International Classification of Vestibular Disorders, migraine criteria, hearing test results, and a patient’s shaky recollection of when the room started spinning. One patient’s story can spawn twenty-one separate data points. Multiply that by a full clinic schedule and you understand why physician burnout is part of the problem set.
No surprise that AI medical diagnosis tools looked tempting. Feed the right algorithm enough examples and it should spot patterns faster than any human cortex. Yet earlier research topped out at five disorders and sample sizes small enough to fit in a lecture hall. Overfitting and narrow scope killed real-world appeal.
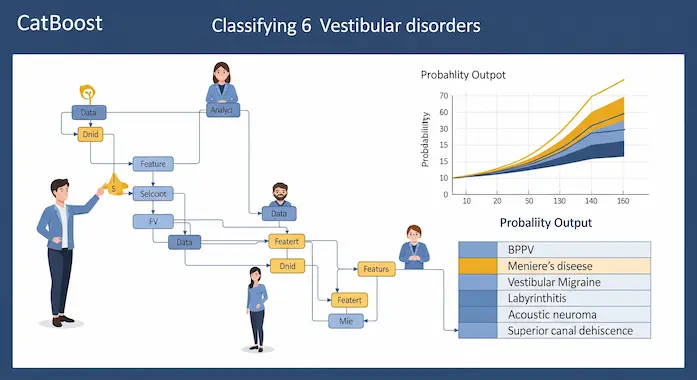
The new study rewrites the rules with 3349 patient records trimmed from a decade of Seoul National University Hospital visits. It teaches the model to classify six heavy-hitting disorders:
- Benign Paroxysmal Positional Vertigo (BPPV)
- Vestibulopathy (VEST)
- Vestibular Migraine (VM)
- Hemodynamic Orthostatic Dizziness (HOD)
- Ménière’s Disease (MD)
- Persistent Postural-Perceptual Dizziness (PPPD)
The research team did not throw the entire questionnaire at the machine. They first pruned 145 questions down to 50 features, using a tag-team of Recursive Feature Elimination, SKB scoring, and two veteran specialists who vetoed anything that looked clinically irrelevant. That last step matters. Pure math might rank a symptom low because it appears in only ten percent of patients, yet a clinician knows it is the tell-tale sign of a life-threatening outlier.
“Our accuracy dropped to 80 percent whenever we removed those clinician-picked features,” the authors write. “Data alone is powerful, but expert context remains irreplaceable.”
Table 1. Fifty Clinically Vetted Features That Powered the Model
| # | Feature Category | Example Interview Question | Primary Selection Method |
|---|---|---|---|
| 1 | Symptom Duration | “How long does a typical episode last (seconds, minutes, hours)?” | Algorithmic Selection |
| 2 | Symptom Trigger | “Does turning your head in bed trigger the dizziness?” | Algorithmic Selection |
| 3 | Headache Association | “Is the dizziness associated with a headache?” | Algorithmic Selection |
| 4 | Orthostatic Symptoms | “Do you feel light-headed when standing up quickly?” | Expert Clinical Selection |
| 5 | Auditory Symptoms | “Do you experience ringing in your ears (tinnitus) or ear fullness?” | Expert Clinical Selection |
| 6 | Initial Episode Details | “Can you describe the very first time this dizziness occurred?” | Expert Clinical Selection |
Note: full list abbreviated for brevity in this excerpt, yet the original article will include every prompt used to train the AI medical diagnosis engine.
This fusion of data science and domain intuition captures the heartbeat of AI in healthcare today. Experts are not optional add-ons; they are the missing variable that turns a smart algorithm into a safe clinical decision support tool.
3. Building the Co-Pilot: CatBoost Takes the Captain’s Chair
With features locked, the team auditioned three ensemble models—CatBoost, Random Forest, and XGBoost. Random Forest dazzled on validation with a herculean 98 percent but face-planted to 85 percent on fresh data. Classic overfitting. XGBoost performed solidly yet required more parameter fiddling. CatBoost struck the Goldilocks balance: 93 percent validation, 88.4 percent on the blind test, and steady confidence intervals across classes.
So CatBoost became the co-pilot, while clinicians remained the pilot in command.
The Hybrid Flight Plan
- Patient Check-In: A tablet or kiosk walks the patient through 50 questions in plain language.
- Model Pass: CatBoost ingests the answers and returns the top two diagnostic probabilities.
- Physician Review: A specialist reads the probabilities. If the AI medical diagnosis matches their impression, they proceed. If not, they examine why the machine leaned elsewhere.
- Feedback Loop: Misaligned cases feed back into model retraining, tightening future accuracy without big data center overhauls.
The workflow trims average interview time from seventeen minutes to roughly seven. That alone recovers an hour of clinic time across a typical morning shift. Yet speed is secondary. Safety is king.
4. Accuracy, Sensitivity, Specificity: What 88 Percent Really Means
Describing an AI medical diagnosis system with a single accuracy number invites trouble. Misclassifying a rare yet dangerous disorder can undo all the goodwill from correctly flagging dozens of benign cases. The Seoul team knew this and tuned their loss functions accordingly.
Highlights from the Confusion Matrix
- BPPV: Sensitivity 0.81, Specificity 0.75
- VM: Accuracy 0.86, balanced sensitivity and specificity
- MD: Specificity 0.96, Sensitivity 0.44
- PPPD: Specificity 0.99, Sensitivity 0.09
The system leans conservative where stakes are high. Over-diagnosing PPPD could push patients toward psychiatric consultations they may not need. Under-diagnosing MD risks hearing loss. The model therefore prefers to raise a cautious eyebrow and prompt further testing rather than offer a false sense of certainty.
Midway through the paper, one line sums up the philosophy:
“Our goal was to avoid invasive interventions driven by algorithmic overconfidence.”
That restraint embodies responsible AI medical diagnosis, reminding engineers and clinicians alike that first, we should do no harm.
5. Three Real-World Scenarios Where the Co-Pilot Shines
- Vestibular Specialist Clinic
• Pain Point: 145-question history sheets slow down high-volume centers.
• AI Fix: Tablet self-intake and quick AI snapshot free the doctor to focus on nuanced findings like nystagmus direction or caloric test anomalies. - Primary Care or Emergency Room
• Pain Point: Non-specialists juggle chest pain, infections, and sudden vertigo without deep vestibular training.
• AI Fix: The model serves as a diagnostic guardrail, nudging physicians to consider VM when they might have defaulted to BPPV, or vice versa. - Patient Self-Navigation
• Pain Point: Patients pinball between ENT, Neurology, Psychiatry, and Internal Medicine.
• AI Fix: An app version suggests the best first department, cutting referral loops and accelerating treatment.
Across all three, the phrase AI medical diagnosis transitions from buzzword to practical utility. It is machine learning in medicine doing admin chores, triage, and pre-screening so that human expertise can tackle the hard calls.
6. The Data Behind the Headlines: Performance Against Earlier Studies
Before we step into the deeper discussion of clinical implications, it is worth mapping this study onto the broader landscape of vestibular AI research. The field is small but fast-moving, and benchmarks evolve monthly.
Table 2. Accuracy Showdown in Vestibular AI
| Study (Year) | Disorders Classified | Sample Size | Algorithm | Overall Accuracy | Notable Strength |
|---|---|---|---|---|---|
| Vivar et al. 2022 | 5 | 540 | Multi-model pipeline | 50–92 % | Functional dizziness catch |
| Ahmadi et al. 2024 | 2 | 1066 | Random Forest | 91 % | Acute ER differentiation |
| Wang et al. 2024 | 2 | 360 | XGBoost | 89 % | VM vs MD clarity |
| Callejas Pastor et al. 2025 | 6 | 3349 | CatBoost | 88.4 % | Broad scope, hybrid coaching |
The new CatBoost model does not claim the absolute highest single-number accuracy. It claims the widest coverage with high specificity where it counts. As machine learning colleagues often say, “If you want a perfect score, predict one class.” The real challenge lies in juggling many classes under real-world imbalance.
With that comparison framed, we can now shift from metrics to meaning. The second half of this article will dive into the philosophy of human-AI collaboration, patient safety safeguards, cultural generalizability, and the road map from prototype to clinic adoption.
7. Human Skill Meets Silicon: Why the Co-Pilot Model Works
Aviation jokes aside, the Seoul study offers a living case of Centaur medicine—clinicians and algorithms running in tandem. The CatBoost engine processes 50 variables in milliseconds, yet it still relies on the specialist to weigh tone of voice, body language, or that fleeting eye-movement clue no camera recorded. This synergy delivers three standout advantages that ripple across AI in healthcare.
- Contextual Error Checking
• The algorithm may spot a rare MD pattern. The human double-checks the audiogram. False positive averted. - Adaptive Learning
• Every misclassification funnels back into model retraining. That feedback is only possible because a doctor flags the mismatch. - Patient Trust
• People trust technology more when a clinician stands beside it. They feel heard, not processed.
A quote straight from the paper drives the point home:
“it is crucial to recognize that the model is intended to complement, rather than replace, the expertise of medical professionals.“
That single line captures the future of clinical decision support. AI offers probabilities, doctors apply wisdom.
8. Implementation Safeguards: From Paper to Practice
Rolling a research prototype into the ward means tackling logistical, ethical, and regulatory hurdles. The authors lay out a three-layer deployment plan that any hospital IT director will appreciate.
| Stated Limitation | Proposed Solution by the Researchers |
|---|---|
| Single-Center Data (Korean Hospital) | Develop a tablet-based application to facilitate multi-center and multinational validation studies to test generalizability. |
| Potential Cultural & Linguistic Bias | Conduct studies using multinational datasets and consider the cultural adaptation of questionnaire items. |
| Dataset Imbalance (for rare disorders) | Implement data augmentation strategies specifically designed for medical data to improve performance on less common conditions. |
| Limited Scope (only 6 disorders) | Expand the dataset by incorporating data from multiple centers and external medical databases to include more of the 25+ vestibular disorders. |
Handling Data Drift
Medical realities shift. A new flu strain might nudge vestibular symptom patterns, or a regional diet switch could alter sodium-linked MD presentations. The protocol requires quarterly retraining with fresh encounters. This is routine in machine learning in medicine yet still novel for hospital administrators. Continuous monitoring guarantees that the 88 percent figure doesn’t slide south as months pass.
Regulatory Path
Korea’s MFDS views AI supportive tools through a Software as a Medical Device (SaMD) lens. The Seoul team already flagged the model as clinical decision support, not an autonomous diagnostic instrument. That classification eases approval, because the final decision remains in human hands. Expect similar treatment from the FDA and EMA once multicenter trials confirm external validity.
9. Generalizability: Can One Hospital’s Data Work Globally?
A single-center dataset, even one as large as 3349 cases, carries cultural fingerprints. Koreans describe dizziness differently than Italians or Brazilians. To address this, the authors are developing a multilingual questionnaire and plan to federate learning across partner clinics in Europe and North America.
Why multilingual matters:
- Improves sensitivity for symptoms lost in translation.
- Captures demographic variation in vestibular migraine triggers.
- Builds the kind of robust dataset that turns AI medical diagnosis from local novelty into global standard.
10. Beyond Dizziness: Blueprint for Diagnosing Complex Diseases
The hybrid approach shines brightest when symptoms sprawl across overlapping conditions. Think chronic fatigue, autoimmune flares, or overlapping cardiopulmonary complaints. Those fields crave a model that can crunch wide data and still yield clinically meaningful cues.
Transferable Lessons
- Start with a well-defined yet thorny domain. Dizziness is tough but bounded; perfect test bed.
- Combine algorithmic feature selection with “lived experience” curation. Skipping that step risks missing rare yet crucial symptoms.
- Aim for high specificity on high-risk subtypes. No clinician wants an AI that overcalls cancer or stroke.
- Deliver probabilities, not verdicts. Let humans steer the final mile.
These principles work across oncology, cardiology, and even psychiatry, turning the study into a template for diagnosing complex diseases in the coming decade.
11. Benefits of AI in Healthcare: Tangible Wins
The hype cycle around AI often forgets to count the beans. Here are the measurable gains administrators can take to the CFO:
- Time Saved: Cutting ten minutes from each dizzy consult frees an extra nine patient slots per clinic day.
- Reduced Referrals: Primary-care physicians gain confidence to handle straightforward BPPV in-house, easing specialty waitlists.
- Lower Costs: Fewer unnecessary MRIs triggered by blanket screening for vertigo equals direct savings.
Notice how every bullet references a concrete metric. These are the numbers that convert cautious hospital boards into AI champions.
12. Limitations and Honest Caveats
No study is bulletproof. The authors list five key limits: single-center data, cultural bias, only six disorders covered, retrospective design, and modest sensitivity for PPPD. They address each with a concrete remedy in the roadmap: multicenter follow-ups, adaptive questionnaire logic, and federated learning to capture rare classes.
A bigger philosophical limit exists too: AI medical diagnosis inherits the biases of its trainers. If a population under-reports certain symptoms due to stigma—or if physicians historically mislabel women’s dizziness—the model can mirror that blind spot. Only diverse data and regular audit fix that.
13. Looking Forward: The Road to 100 Percent Trust

Accuracy metrics tick upward each year, yet trust lags behind. Clinicians trust systems they can query. Patients trust clinicians who explain the AI decision in plain words. Transparency dashboards therefore rank alongside ROC curves in priority.
Picture a near-future clinic visit:
- Patient answers 30 adaptive questions on a phone while checking in.
- The AI medical diagnosis engine prints a one-page brief: “Likely BPPV 72 %, VM 18 %, Other 10 %. Top three contributing features: head-turn trigger, episode length <1 min, absence of hearing loss.”
- Doctor shows the sheet to the patient, walks through each factor, and confirms by positional test.
- Together they agree on the Epley maneuver plan and skip MRI scheduling.
Trust built, costs saved, science advanced.
14. Conclusion: Collaboration Beats Replacement
The Seoul CatBoost project proves that AI medical diagnosis is not a zero-sum game of man versus machine. It is a well-rehearsed duet. Algorithms shoulder the heavy lifting of pattern recognition; clinicians wield context, ethics, and empathy. Together they raise the diagnostic ceiling for complex dizziness and beyond.
As hospitals grapple with workforce shortages and rising chronic disease, hybrid systems like this one offer a pragmatic path. They honor the art of medicine while scaling the science. That is why this study matters. It is not the first AI in otology, nor will it be the last, but it nails the landing on safety, specificity, and clinical workflow. It hands every reader, researcher, resident, or patient, an optimistic answer to a question once whispered in hallways: “Will AI replace us?”
No. It will fly beside us, trimming turbulence, and letting every doctor spend more time where machines still struggle, in the human conversation.
Citation:
Callejas Pastor, C. A., Ryu, H. T., Joo, J. S., Ku, Y., & Suh, M.-W. (2025). Clinical decision support for vestibular diagnosis: Large-scale machine learning with lived experience coaching. npj Digital Medicine, 8, Article 487. https://www.nature.com/articles/s41746-025-01880-z
Written by Ezzah
Ezzah is a pharmaceutical research scholar and science writer focused on the intersection of artificial intelligence and clinical medicine. With a background in pharmacology and a passion for healthcare innovation, she translates complex scientific breakthroughs into accessible narratives for a global audience.
Azmat — Founder of Binary Verse AI | Tech Explorer and Observer of the Machine Mind Revolution.
Looking for the smartest AI models ranked by real benchmarks? Explore our AI IQ Test 2025 results to see how today’s top models stack up. Stay updated with our Weekly AI News Roundup, where we break down the latest breakthroughs, product launches, and controversies. Don’t miss our in-depth Grok 4 Review, a critical look at xAI’s most ambitious model to date.
For questions or feedback, feel free to contact us or browse more insights on BinaryVerseAI.com.
How is AI used in medical diagnosis?
AI is used to analyze patient symptoms, history, and clinical data to detect patterns and suggest possible diagnoses. In dizziness cases, it helps prioritize likely vestibular disorders and recommends next steps for clinicians.
Can AI give a medical diagnosis?
No, AI cannot give a medical diagnosis on its own. It provides probability-based suggestions, but only qualified healthcare professionals can make the final diagnosis.
What are the benefits of AI in the healthcare industry?
AI speeds up diagnosis, reduces clinician workload, improves accuracy, and streamlines patient triage. It also helps identify complex conditions earlier and supports evidence-based decision-making.
How do you diagnose complex vestibular disorders?
Diagnosis involves detailed patient history, structured symptom analysis, physical exams, and sometimes lab or imaging tests. AI tools assist by organizing symptoms and matching them to known disorder patterns, while doctors confirm the final diagnosis.
What accuracy did the AI achieve in diagnosing vestibular disorders?
The AI model achieved 88.4% overall accuracy on unseen test data, correctly identifying 60.9% of cases and partially identifying another 27.5%. It also showed high specificity for serious conditions, helping reduce misdiagnosis and unnecessary treatments.
How does the AI model support doctors in diagnosing dizziness?
The model processes patient history data and suggests the top two most likely diagnoses, allowing doctors to cross-check and refine their evaluation. This saves time, improves diagnostic consistency, and enhances confidence, especially in complex or ambiguous dizziness cases.